





")



You’re mid-stride during a morning jog when suddenly, a sharp, tearing sensation rips through your heel—like a rubber band snapping under pressure. You hear a distinct pop, stumble forward, and collapse to the ground, unable to put weight on your foot. This isn’t just a flare-up of plantar fasciitis. What you’ve likely experienced is a ruptured plantar fascia, a severe and often misdiagnosed injury that demands immediate attention. Unlike the gradual onset of heel pain associated with plantar fasciitis, a rupture strikes suddenly and violently, leaving behind swelling, bruising, and significant functional loss. Recognizing the signs of a ruptured plantar fascia early is crucial to preventing long-term complications like arch collapse, chronic instability, or even surgery. In this guide, you’ll learn how to distinguish a rupture from common heel pain, what risk factors increase your odds, and exactly what to do if you suspect a tear.
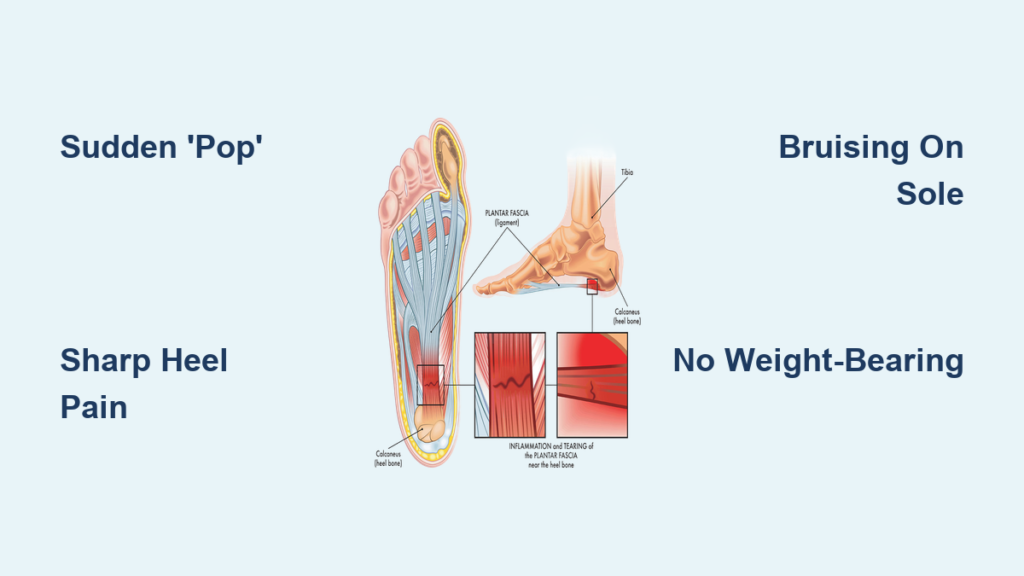
Sudden “Pop” and Acute Pain in the Heel
Immediate Tearing or Stabbing Sensation
One of the most definitive signs of a ruptured plantar fascia is an instant, sharp tearing or stabbing pain in the heel or arch. This isn’t a dull ache that builds over time—it hits without warning, typically during high-impact activity like sprinting, jumping, or forcefully pushing off the foot. Many patients describe it as feeling like they were kicked in the heel or stepped on a piece of glass. The pain stems from a macroscopic tear in the thick connective tissue that supports the foot’s arch, most commonly affecting the central band near its attachment to the heel bone.
Unlike plantar fasciitis, which worsens with rest and improves slightly with movement, a rupture causes severe, disabling pain from the first moment. If you’re active and experience sudden heel pain during exercise, especially with a history of heel discomfort, consider a rupture a strong possibility.
Hearing or Feeling a “Pop” at the Moment of Injury
A hallmark symptom of plantar fascia rupture is hearing or feeling a loud “pop” at the exact moment of injury. This occurs when the fascia fibers snap under excessive tension, usually during forceful dorsiflexion—when the toes are pulled upward rapidly. The sound isn’t imagined; it’s a physical manifestation of tissue failure.
If you experience both a sudden, sharp pain and an audible or sensory “pop”, treat it as a medical red flag. Do not attempt to walk it off or continue activity. Immediate rest, elevation, and medical evaluation are essential to prevent worsening damage.
Swelling and Bruising on the Sole of the Foot

Rapid Development of Swelling
Within minutes to hours after the injury, swelling appears on the bottom of the foot, particularly in the arch and heel. The area may feel warm, tender, and inflamed. This reaction is the body’s natural response to internal tissue damage and bleeding.
While plantar fasciitis rarely causes noticeable swelling, a rupture triggers significant inflammation due to the physical tear in the fascia. The presence of swelling—especially on the plantar surface—is a strong indicator of structural damage.
Visible Bruising (Ecchymosis) Under the Foot
One of the clearest visual clues of a rupture is bruising on the sole of the foot. Blood from the torn tissue leaks into surrounding areas and often becomes visible within 24 to 48 hours. The bruise may start near the heel and spread toward the midfoot or toes as blood tracks along tissue planes.
Crucially, bruising on the bottom of the foot is extremely rare in plantar fasciitis. If you notice purple, blue, or yellow discoloration under your foot following sudden heel pain, especially with a “pop,” seek medical attention immediately. This combination is a near-certain sign of a rupture.
Inability to Bear Weight on the Affected Foot
Severe Limping or Complete Weight-Bearing Failure
A ruptured plantar fascia severely compromises your ability to walk. Most people find it painful or impossible to stand or walk on the injured foot. Even putting light pressure down can cause intense pain.
Common signs include:
– A severe limp or refusal to bear weight
– Inability to push off the foot during walking
– Difficulty standing on your toes
This functional impairment happens because the plantar fascia acts like a bowstring, supporting the arch and absorbing shock during gait. When it tears, that support is lost, leading to instability and pain.
Loss of Push-Off Strength and Propulsion
The plantar fascia plays a key role in the windlass mechanism, which tightens the arch when you lift your heel and push off during walking. A rupture disrupts this mechanism, resulting in weakness, instability, and reduced propulsion.
If you can’t walk without crutches or a boot after sudden heel pain—especially with a “pop”—a rupture is highly likely.
Physical Evidence of Tissue Damage

Palpable Gap or Depression in the Arch
In cases of complete rupture, a skilled clinician may detect a visible or palpable defect along the plantar fascia. This gap is often felt in the mid-arch or near the heel. To check, gently press along the inner arch from the heel to the ball of the foot. A soft spot or depression where firm tissue should be may indicate a full-thickness tear.
While not always present, a palpable gap is a strong clinical sign of significant structural damage.
Flattening of the Foot Arch
Without the support of an intact plantar fascia, the longitudinal arch can collapse, leading to an acquired flatfoot deformity. You might notice your foot appears flatter when standing, especially compared to the unaffected side.
This change in foot structure can persist if untreated and may lead to long-term biomechanical issues, including tendon strain and joint pain.
Key Risk Factors That Increase Your Chances

Chronic Plantar Fasciitis
Long-standing plantar fasciitis is the top risk factor for rupture. Repeated microtears and inflammation weaken the fascia, making it vulnerable to a sudden, complete tear.
If you’ve had heel pain for months and suddenly feel a “pop,” suspect a rupture immediately.
Corticosteroid Injections
While cortisone shots can relieve plantar fasciitis pain, they weaken collagen fibers in the fascia. Studies show that ruptures often occur within weeks of an injection.
Medical guidelines now recommend limiting cortisone shots to one or two per foot and avoiding them in active individuals.
Fluoroquinolone Antibiotics
Medications like Ciprofloxacin (Cipro) and Levofloxacin (Levaquin) carry an FDA “Black Box” warning for tendon and ligament ruptures. These antibiotics impair collagen synthesis and can cause spontaneous tears—even without trauma.
If you’re on a fluoroquinolone and develop sudden foot pain, stop the medication and contact your doctor immediately.
Tight Calf Muscles and High-Impact Sports
Limited ankle dorsiflexion—often due to tight calf muscles—increases strain on the plantar fascia. Combine that with sports like basketball, tennis, or sprinting, and the risk rises significantly.
Athletes should prioritize calf stretching and gradual training progression.
How Doctors Diagnose a Ruptured Plantar Fascia
Clinical History and Physical Exam
Doctors ask key questions:
– Did you hear a “pop”?
– Was the pain sudden or gradual?
– Were you active at the time?
– Do you have a history of plantar fasciitis or steroid injections?
They’ll check for tenderness, swelling, bruising, weight-bearing ability, and arch structure.
MRI: The Most Accurate Diagnostic Tool
MRI is the gold standard for confirming a rupture. It clearly shows:
– Location and extent of the tear
– Retraction of the torn fascia
– Surrounding edema and soft tissue damage
It also helps rule out stress fractures or tendon injuries.
Ultrasound: Real-Time Imaging Option
Musculoskeletal ultrasound is a cost-effective, dynamic alternative. A trained sonographer can:
– Visualize fascial discontinuity
– Detect thickening or retraction
– Perform dynamic imaging during foot movement
It’s excellent for monitoring healing.
X-Ray: Rules Out Fractures
While X-rays can’t show soft tissue tears, they help exclude fractures, heel spurs, or bone abnormalities. In chronic cases, they may reveal arch collapse.
Immediate Care: What to Do in the First 72 Hours
Rest and Non-Weight-Bearing
Stop all activity. Use crutches or a walker. Stay non-weight-bearing for 2–3 weeks to allow healing.
Ice, Elevation, and Compression
Apply ice for 15–20 minutes every 2–3 hours. Keep the foot elevated above heart level. Use a compression wrap (not too tight).
Transition to a Walking Boot
Once swelling decreases, wear a removable walking boot (cam walker) for 4–6 weeks to immobilize the foot and reduce strain.
Final Note: A ruptured plantar fascia is a serious injury that mimics severe plantar fasciitis but requires a different approach. Sudden “pop,” sharp pain, bruising, and inability to walk are red flags. Seek care the same day—delayed treatment increases the risk of long-term complications. With prompt diagnosis, proper immobilization, and rehabilitation, most people regain full function. The key is recognizing the signs early and acting fast.



